Introduction and objective: Acute coronary syndrome (ACS) is a cardiac emergency, and significant progress has been made in its management in Togo. This study aimed to describe coronary lesions in ACS patients and aspects of myocardial revascularisation. Materials and methods: This cross-sectional study was conducted at Dogta-Lafiè Hospital and Autel d'Elie Private Hospital in Lomé over four years and six months (January 2021 to June 2025). All patients who underwent coronary angiography for acute coronary syndrome during the study period were included. Results: Out of 298 requests for coronary angiography for ACS, 184 patients underwent the procedure. The coronary angiography performance rate was 61.75%. The mean patient age was 57.9 ± 12.6 years, with a male predominance (sex ratio 1.8). ST-segment elevation myocardial infarction (STEMI) accounted for 62.5%. Significant coronary lesions were found in 161 patients (87.5%), which were significantly more prevalent in STEMI than in non-ST-segment elevation acute coronary syndrome (NSTE-ACS) (p = 0.0001). Depending on the complexity of the coronary lesions, type B lesions were significantly more prevalent in STEMI than in NSTE-ACS, while type C lesions were more prevalent in NSTE-ACS. Percutaneous coronary intervention was performed on only 86 patients (46.74% of those who underwent coronary angiography for ACS and 67.19% of those for whom percutaneous coronary intervention was indicated). Percutaneous coronary intervention was performed in 51 patients with STEMI (46.79%), including 13 cases of primary percutaneous coronary intervention (25.49%). Coronary artery bypass grafting was performed in 50% of patients for whom it was indicated. Two patients (1.56%) died from complications following angioplasty due to ventricular fibrillation. Conclusion: Coronary angiography is rarely performed in ACS, but it allows assessment of lesions. The rate of myocardial revascularisation also remains.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
Acute coronary syndrome (ACS) is a cardiac emergency for which well-established treatment guidelines exist
[1]
Collet JP, Thiele H, Barbato E, Barthélémy O, Bauersachs J, Bhatt DL, et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: The Task Force for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J 2021; 42(14): 1289‑367.
Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. 2018; 39(2): 119‑77.
. There are two forms of ACS: ST-segment elevation myocardial infarction (STEMI) and non-ST-segment elevation acute coronary syndrome (NSTE-ACS). ACS is an unstable form of ischaemic heart disease, the leading cause of death worldwide
[3]
Global Health Estimates: Life expectancy and leading causes of death and disability [Internet]. Available from:
. A study covering the period from 2002 to 2016 at the Institute of Cardiology in Abidjan found that the prevalence of ACS was 14.9%
[4]
Yao H, Ekou A, Brou I, Niamkey T, Koffi F, Tano S, et al. Evolution of epidemiology and management of acute coronary syndromes in Abidjan: A cross-sectional study of 1011 patients. Ann Cardiol Angéiologie 2022; 71(3): 130‑5.
. Remarkable progress has been made in the management of ACS over the past 15 years in sub-Saharan Africa, with the development of specialist teams and interventional cardiology units. This progress has resulted in improved ACS management
[6]
N’Guetta R, Ekou A, Yao H, Anzouan-Kacou JB, Gérardin B, Pillière R, et al. Percutaneous coronary intervention in the management of acute coronary syndromes in Ivory Coast: Challenges and outcomes. Ann Cardiol Angéiologie 2018; 67(4): 244‑9.
Diop IB, Manga S, Dioum M, Leye M, Ba K, Bindia D, et al. Inaugural experience of interventional cardiology at Jacques Bessol Coronary Angiography Centre of the University Hospital of Fann (Dakar): Outcomes, difficulties and perspectives. Cardiol Trop 2017; 147: 1‑7.
[6, 7]
. However, in Togo, where the hospital prevalence increased from 3.5% to 5.87% and the mortality rate fell from 10% to 6.25% between 2018 and 2025
[8]
Pessinaba S, Atti YDM, Yayehd K, Simwétaré MBF, Kaziga W, Afassinou YM, et al. Acute coronary syndromes: epidemiological, clinical, paraclinical and therapeutic characteristics at the Campus teaching hospital of Lome, Togo. Médecine Santé Trop 2018; 28(3): 285‑8.
Afassinou YM, Abdou S, Pessinaba S, Kaziga DD W, Atta B, et al. Management of Acute Coronary Syndromes in the Era of Interventional Cardiology in Togo. World J Cardiovasc Dis 2025; 15(5): 254-69.
, coronary angiographic lesions in ACS remain poorly understood. The development of interventional cardiology activities over the past six years has enabled comprehensive management of coronary artery disease, particularly ACS
[10]
Afassinou YM, Pessinaba S, Ehlan KE, Magoua NK, Borgatia A, Pio M, et al. From hypoglycemia to myocardial infarction: another particularity of diabetes. Sang Thromb Vaiss 2023; 35(1): 25‑7.
Afassinou Y, Edorh L, Pessinaba S, Atta B, Sodou A, Oloude N, et al. Spontaneous Dissection of the Coronary Artery: A Cause of Myocardial Infarction not to be forgotten in the Young Subject. Ann Vasc Med Res 2023; 10(1): 1‑4.
[10, 11]
. This study aims to describe coronary lesions in ACS patients in Lome and aspects of myocardial revascularisation.
2. Material and Methods
2.1. Type and Setting of the Study
The study was conducted in two hospitals in Togo that specialise in the interventional management of coronary artery disease. The hospitals were Dogta-Lafiè Hospital and Autel d'Elie Private Hospital, both in Lomé. The cross-sectional study was conducted over a period of four years and six months, from 1 January 2021 to 30 June 2025.
2.2. Study Population
The study population consisted of patients who were referred for coronary angiography, either with or without percutaneous coronary intervention.
All consecutive patients who underwent coronary angiography with or without percutaneous coronary intervention for ACS during the study period were included in this study. ACS was diagnosed based on a set of suggestive clinical manifestations, such as chest pain or equivalents (dyspnoea, epigastric pain, or pain in the upper limbs), in conjunction with electrocardiographic changes and/or elevated troponin levels. Electrocardiographic changes included new ST-segment elevation at the J-point in at least two contiguous leads, new bundle-branch block, ST-segment depression, and T-wave changes. Troponin I was the only marker measured.
2.3. Data Collection
Data collection was performed using a pre-established Excel database based on medical records, as well as on coronary angiography and angioplasty images from the CathLabs archiving system or compact discs. The interventional cardiology devices used were the CANON ALPHENIX 001A, commissioned on 11 September 2023 for the Dogta-Lafiè Hospital, and the SHIMADZU, commissioned in September 2019 for the Autel d'Elie Private Hospital. The parameters studied were socio-demographic factors (age, gender and health insurance status), cardiovascular risk factors, acute coronary syndrome (ACS) presentation, characteristics of coronary angiographic lesions, myocardial revascularisation and immediate outcomes (results and complications). Hypertension was defined as systolic blood pressure (BP) of ≥140mmHg, diastolic BP of ≥90mmHg or documented antihypertensive treatment. Obesity was defined as a body mass index (BMI) of 30.0kg/m² or higher. For the purposes of this study, diabetes mellitus was defined as having two fasting blood glucose levels of >1.26 g/L and/or a documented medical history of diabetes or diabetes treatment. The threshold values for dyslipidaemia are those of the National Cholesterol Education Programme (NCEP)
[12]
Grundy SM, Cleeman JI, Daniels SR, Donato KA, Eckel RH, Franklin BA, et al. Diagnosis and management of the metabolic syndrome: an American Heart Association/National Heart, Lung, and Blood Institute Scientific Statement. Circulation 2005; 112(17): 2735‑52.
. Smoking was identified as a risk factor if it was currently present or had ceased within the last three years. A family history of coronary artery disease was defined as its presence in the patient's family.
An interventional cardiologist reviewed the coronary angiography and angioplasty images. Quantitative coronary angiography was used to calculate the vessel diameter and degree of luminal narrowing. All images were calibrated according to the guide catheter used. Lesions were classified according to the number of vessels involved (single-vessel, two-vessel or three-vessel) and according to their complexity (American College of Cardiology/American Heart Association classification
[13]
Ryan T, Faxon D, Gunnar R, Kennedy J, King S, Loop F, et al. Guidelines for percutaneous transluminal coronary angioplasty. A report of the American College of Cardiology/American Heart Association Task Force on Assessment of Diagnostic and Therapeutic Cardiovascular Procedures (Subcommittee on Percutaneous Transluminal Coronary Angioplasty). Circulation 1988; 78(2): 486‑502.
) in the presence of obstructive coronary artery disease. Significant coronary artery disease was defined as ≥50% narrowing of the diameter of at least one major epicardial vessel (≥2.25mm in diameter). Therefore, a lesion was considered significant if it was stenotic and obstructed at least 70% of the coronary artery lumen. An intermediate lesion was defined as a stenotic lesion obstructing the coronary artery lumen by between 50% and 70%. A lesion was considered non-significant if there was less than 50% obstruction of the coronary artery lumen. A common trunk lesion was considered significant if there was significant coronary artery disease (≥50%) on the common trunk. Therapeutic indications (percutaneous coronary intervention (PCI), coronary artery bypass grafting (CABG), or medical treatment alone) were based on urgency, complexity of coronary lesions, patient characteristics (age, frailty, diabetes, and left ventricular systolic function), local expertise (technical skills and available equipment), and patients' financial resources
[14]
Neumann FJ, Sousa-Uva M, Ahlsson A, Alfonso F, Banning AP, Benedetto U, et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. EuroIntervention J Eur Collab Work Group Interv Cardiol Eur Soc Cardiol 2019; 14(14): 1435‑534.
The text was processed using Microsoft Word 2016. Data analysis was performed using Epi Info version 3.5.4. A Mantel–Haenszel chi-squared test was performed with a significance threshold of p < 0.05, and a Fisher's exact test was performed for sample sizes of less than five. These tests were employed to compare variables in both univariate and multivariate analyses.
2.5. Ethical Considerations
Data confidentiality was guaranteed. Patient names do not appear in any documents relating to the results of this study. Ethical approval for the study was obtained from the Health Ethics Committee of the Faculty of Health Sciences at the University of Lome. The study was conducted in accordance with the International Conference on Harmonisation of Good Clinical Practice guidelines and the Declaration of Helsinki.
3. Results
3.1. Epidemiological Characteristics
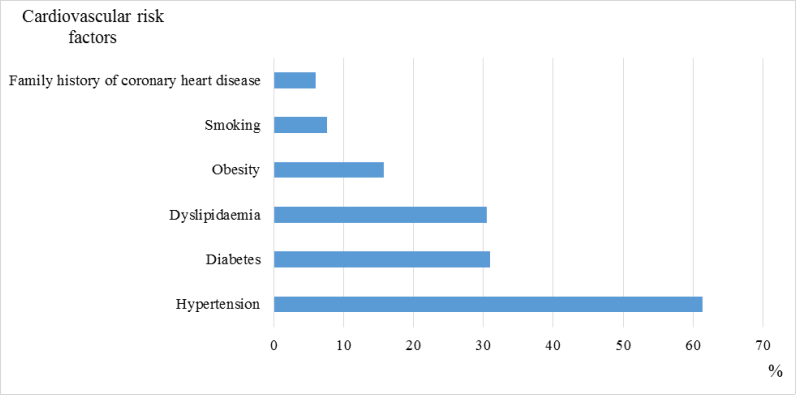
During the study period, coronary angiography was performed on 184 out of 298 patients with ACS who requested it. The performance rate of coronary angiography in ACS patients was 61.75%. The mean age of the patients was 57.9 ± 12.6 years, and there was a male predominance (sex ratio 1.8). Health insurance covering coronary angiography was available for 36 patients (19.57%). Hypertension was identified as a cardiovascular risk factor in 61.41% of patients. A family history of coronary heart disease was also identified (Figure 1).
Figure 1. Cardiovascular risk factors in patients undergoing coronary angiography for ACS.
ACS presented as STEMI in 115 patients (62.5%) and as NSTE-ACS in 69 patients (37.5%). For patients with STEMI, the time to admission was greater than 24 hours in 56.5%. Among patients referred for STEMI, thrombolysis was performed in 32 patients (17.39%) before coronary angiography.
3.2. Coronary Lesions and Revascularisation Methods
Significant coronary lesions were found in 161 patients (87.5%). These lesions were significantly more prevalent in patients with STEMI than in those with NSTE-ACS (p = 0.0001) (Table 1). Two-vessel disease were significantly more prevalent in patients with STEMI (p = 0.0199). The left anterior descending artery and the right coronary artery were affected in 64.67% and 54.89% of cases, respectively. The left main trunk was also the site of significant lesions (Table 2).
Depending on the severity and complexity of the coronary lesions, type B and type C lesions were present in 39.13% and 35.40% of cases, respectively. Type B lesions were significantly more prevalent in STEMI than in NSTE-ACS, whereas type C lesions were more prevalent in NSTE-ACS (Table 3).
Table 1. Type of coronary lesions according to ACS presentation.
ACS
STEMI
NSTE-ACS
p
n=184
n=115
n=69
Significant lesions
161 (87.50)
109 (94.78)
52 (75.36)
0.0001
One-vessel disease
62 (33.70)
42 (36.52)
20 (28.99)
0.2964
Two-vessel disease
41 (22.28)
32 (27.83)
9 (13.04)
0.0199
Three-vessel disease
58 (31.52)
35 (30.43)
23 (33.33)
0.6828
Table 2. Sites of significant lesions found.
n
Left main
5
2.71
Left anterior descending artery
1
64.67
Proximal Left anterior descending artery
51
27.71
Middle Left anterior descending artery
7
42.93
Distal Left anterior descending artery
26
14.13
Circumflex artery
68
36.96
Proximal circumflex artery
23
12.50
Middle circumflex artery
52
28.26
Distal circumflex artery
16
8.70
Bissectrix artery
13
7.07
Right coronary artery
101
54.89
Proximal right coronary artery
64
34.78
Middle right coronary artery
53
28.80
Distal right coronary artery
22
11.96
Table 3. Complexity and severity of significant coronary lesions.
STEMI
NSTE-ACS
p
n=109
n=52
Type A
28 (25.68)
13 (25.00)
0.9255
Type B
48 (44.04)
15 (28.85)
0.0656
Type C
33 (30.28)
24 (46.15)
0.0495
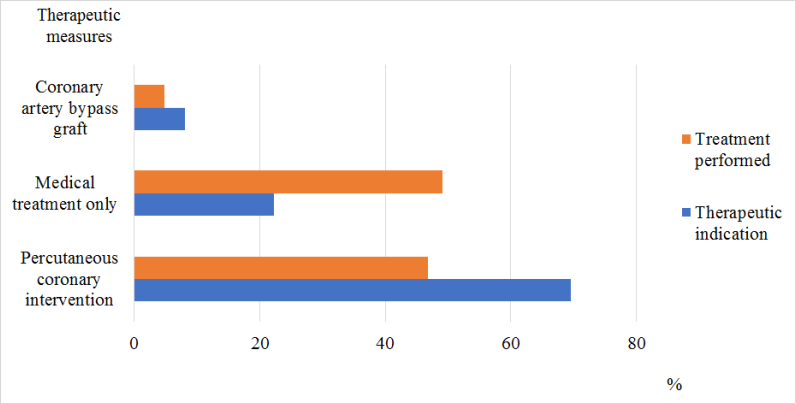
PCI was indicated in 128 patients (69.56%). CABG was indicated in 15 patients (8.15%). However, PCI was only performed on 86 patients, representing 46.74% of those who underwent coronary angiography for ACS and 67.19% of those for whom PCI was indicated. PCI was performed in 51 patients with STEMI (46.79%), including 13 cases of primary PCI (25.49%). CABG was performed on nine patients (50% of those indicated for bypass grafting) (Figure 2).
Figure 2. Therapeutic indication and treatment performed in the ACS.
Two patients (1.56%) experienced complications following percutaneous coronary intervention. One case of distal coronary perforation and one case of haematoma at the puncture site. Two patients (1.56%) died due to fatal ventricular fibrillation.
4. Discussion
4.1. Keys Findings
The coronary angiography rate was 61.75% for ACS patients. This is lower than the results of the French FAST-MI 2010 registry, which found coronary angiography rates of 96% and 91% in STEMI and NSTE-ACS, respectively
[15]
Belle L, Cayla G, Cottin Y, Coste P, Khalife K, Labèque JN, et al. French Registry on Acute ST-elevation and non−ST-elevation Myocardial Infarction 2015 (FAST-MI 2015). Design and baseline data. Arch Cardiovasc Dis 2017; 110(6): 366‑78.
. However, this rate is relatively high compared to the 44.1% reported by Yao in Côte d'Ivoire
[17]
Yao H, Ekou A, Niamkey TJ, Soya EK, Aboley E, N’Guetta R. Coronary lesions in black African patients with acute coronary syndromes. Pan Afr Med J 2019; 32(104).
. Despite these differences, we are all faced with the discrepancy between patients' limited financial resources and the relatively high cost of coronary angiography in our countries. This is compounded by low health insurance coverage (19.57%) in our study and a lack of free emergency care facilities, which endangers patients' lives.
The average age of patients was 57.9 ± 12.6 years, with a predominance of males (sex ratio of 1.8). The young age of the patients in our study is consistent with other African studies
[17]
Yao H, Ekou A, Niamkey TJ, Soya EK, Aboley E, N’Guetta R. Coronary lesions in black African patients with acute coronary syndromes. Pan Afr Med J 2019; 32(104).
Schamroth C, ACCESS South Africa investigators. Management of acute coronary syndrome in South Africa: insights from the ACCESS (Acute Coronary Events - a Multinational Survey of Current Management Strategies) registry. Cardiovasc J Afr 2012; 23(7): 365‑70.
Isezuo S, Sani MU, Talle A, Johnson A, Adeoye AM, Ulgen MS, et al. Registry for Acute Coronary Events in Nigeria (RACE-Nigeria): Clinical Characterization, Management, and Outcome. J Am Heart Assoc 2022; 11(1): e020244.
, where programmes combat non-communicable diseases and the hospital system allows for a longer life expectancy. High blood pressure was found to be the main cardiovascular risk factor in 61.41% of cases, as in the Yao series
[17]
Yao H, Ekou A, Niamkey TJ, Soya EK, Aboley E, N’Guetta R. Coronary lesions in black African patients with acute coronary syndromes. Pan Afr Med J 2019; 32(104).
Yao H, Ekou A, Niamkey TJ, Soya EK, Aboley E, N’Guetta R. Coronary lesions in black African patients with acute coronary syndromes. Pan Afr Med J 2019; 32(104).
, the presentation of ACS was dominated by STEMI. In 56.50% of cases, the time to admission for STEMI was greater than 24 hours. Various studies have demonstrated the detrimental effect of long times to admission for ACS on effective management
[4]
Yao H, Ekou A, Brou I, Niamkey T, Koffi F, Tano S, et al. Evolution of epidemiology and management of acute coronary syndromes in Abidjan: A cross-sectional study of 1011 patients. Ann Cardiol Angéiologie 2022; 71(3): 130‑5.
Ticolat, P, Bertrand, E, Baeabe P, Bouramoue, C, Burdin, J, Diouf, S et al. Aspects épidémiologiques de la maladie coronaire chez le Noir Africain : à propos de 103 cas. Résultats de l’enquête multicentrique prospective CORONAFRIC. Cardiol Trop. 1991; 17: 7‑20.
[4, 5, 20]
.
Significant coronary lesions were found in 161 patients (87.5%). These lesions were significantly more prevalent in STEMI patients than in NSTE-ACS patients (p=0.0001). Our results are similar to those of Yao et al
[17]
Yao H, Ekou A, Niamkey TJ, Soya EK, Aboley E, N’Guetta R. Coronary lesions in black African patients with acute coronary syndromes. Pan Afr Med J 2019; 32(104).
. NSTE-ACS can mimic other conditions, which could explain why fewer lesions were found in NSTE-ACS patients than in STEMI patients. Two-vessel disease was significantly more prevalent in patients with STEMI (p = 0.0199). Type B and type C lesions were found in 39.13% and 35.40% of cases, respectively. Type B lesions were significantly more prevalent in STEMI than in NSTE-ACS, while type C lesions were more prevalent in NSTE-ACS. Therefore, our patients present with specific characteristics in terms of the number of coronary arteries affected and the complexity of the lesions, whether they have STEMI or NSTE-ACS, as reported in other studies
[17]
Yao H, Ekou A, Niamkey TJ, Soya EK, Aboley E, N’Guetta R. Coronary lesions in black African patients with acute coronary syndromes. Pan Afr Med J 2019; 32(104).
Shavadia J, Yonga G, Otieno H. A prospective review of acute coronary syndromes in an urban hospital in sub-Saharan Africa. Cardiovasc J Afr 2012; 23(6): 318‑21.
. The left anterior descending artery and the right coronary artery were affected in 64.67% and 54.89% of cases, respectively. Diop in Senegal found the anterior interventricular artery to be responsible for ACS in 49% of cases, the circumflex artery in 40%, and the right coronary artery in 41%
[7]
Diop IB, Manga S, Dioum M, Leye M, Ba K, Bindia D, et al. Inaugural experience of interventional cardiology at Jacques Bessol Coronary Angiography Centre of the University Hospital of Fann (Dakar): Outcomes, difficulties and perspectives. Cardiol Trop 2017; 147: 1‑7.
[7]
.
PCI was performed in only 86 patients (46.74% of those who underwent coronary angiography for ACS and 67.19% of those for whom PCI was indicated). This is a higher rate than that reported by Yao, who found a percutaneous coronary intervention rate of 22.6% in ACS patients
[4]
Yao H, Ekou A, Brou I, Niamkey T, Koffi F, Tano S, et al. Evolution of epidemiology and management of acute coronary syndromes in Abidjan: A cross-sectional study of 1011 patients. Ann Cardiol Angéiologie 2022; 71(3): 130‑5.
. The PCI rate is also higher than in Diop's study
[7]
Diop IB, Manga S, Dioum M, Leye M, Ba K, Bindia D, et al. Inaugural experience of interventional cardiology at Jacques Bessol Coronary Angiography Centre of the University Hospital of Fann (Dakar): Outcomes, difficulties and perspectives. Cardiol Trop 2017; 147: 1‑7.
[7]
. This difference can be explained by the fact that our study focused on ACS, whereas Diop's study included all coronary diseases. PCI was performed in 51 patients with STEMI (46.79%), of whom 13 (25.49%) underwent primary PCI. CABG was performed in nine patients (50% of indications). Complications following PCI were non-lethal in 1.56% of cases and lethal in the same proportion. The low rate of revascularisation with PCI and surgery is primarily due to financial difficulties experienced by patients. The cost of a PCI procedure ranges from 2,130.24 to 2,485.28 USD. Interventional cardiology procedures are not covered by the universal health insurance scheme, which covers most of the population. Furthermore, CABG is not performed in Togo. Patients must be evacuated abroad at a minimum cost of around 12,426.40 USD. This is significant when we consider that the guaranteed minimum wage in Togo is just 93.20 USD, and that the poverty rate remains high at 53.7%
[22]
UNDP. Togo Sustainable Development Forum Report 2017 | United Nations Development Programme [Internet]. 2017 Available at:
. A second factor contributing to the low rate of myocardial revascularisation in ACS patients is delayed admission for revascularisation once myocardial necrosis has already set in.
4.2. Study Limitations
The weakness of this study is its small sample size. However, the study's merit lies in its provision of important data on lesions encountered in ACS in Togo and on myocardial revascularisation in its aftermath. This is a young field and this work provides an overview of interventional management in ACS which is expected to improve and develop in the coming years.
The severity of the lesions was assessed solely on the basis of angiography, which restricts the evaluation, given the contribution of intracoronary imaging techniques, such as intracoronary ultrasound (IVUS) and optical coherence tomography (OCT). Furthermore, fractional flow reserve could have provided more accurate information on the significance of certain lesions. This could have impacted decisions regarding myocardial revascularisation.
5. Conclusion
This cross-sectional study aimed to describe coronary lesions in ACS patients in Lome, as well as aspects of myocardial revascularisation. The rate of coronary angiography in ACS patients was low. The most common form of ACS was STEMI, and significant coronary lesions were more prevalent in this form. The most prevalent lesion types were one-vessel and three-vessel diseases. Type B lesions were more prevalent in STEMI, while type C lesions were more prevalent in NSTE-ACS. The PCI and CABG rates were low compared to the indications. Public authorities must be urged not only to include interventional cardiology procedures in the universal health insurance coverage package, but also to establish a system of free care for coronary emergencies.
Abbreviations
ACS
Acute Coronary Syndrome
STEMI
ST-segment Elevation Myocardial Infarction
NSTE-ACS
Non-ST-segment Elevation Acute Coronary Syndrome
BP
Blood Pressure
PCI
Percutaneous Coronary Intervention
CABG
Coronary Artery Bypass Grafting
IVUS
Intracoronary Ultrasound
OCT
Optical Coherence Tomography
Acknowledgments
The authors would like to thank the management of both hospitals for their cooperation.
Collet JP, Thiele H, Barbato E, Barthélémy O, Bauersachs J, Bhatt DL, et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: The Task Force for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J 2021; 42(14): 1289‑367.
Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. 2018; 39(2): 119‑77.
Yao H, Ekou A, Brou I, Niamkey T, Koffi F, Tano S, et al. Evolution of epidemiology and management of acute coronary syndromes in Abidjan: A cross-sectional study of 1011 patients. Ann Cardiol Angéiologie 2022; 71(3): 130‑5.
N’Guetta R, Ekou A, Yao H, Anzouan-Kacou JB, Gérardin B, Pillière R, et al. Percutaneous coronary intervention in the management of acute coronary syndromes in Ivory Coast: Challenges and outcomes. Ann Cardiol Angéiologie 2018; 67(4): 244‑9.
Diop IB, Manga S, Dioum M, Leye M, Ba K, Bindia D, et al. Inaugural experience of interventional cardiology at Jacques Bessol Coronary Angiography Centre of the University Hospital of Fann (Dakar): Outcomes, difficulties and perspectives. Cardiol Trop 2017; 147: 1‑7.
[8]
Pessinaba S, Atti YDM, Yayehd K, Simwétaré MBF, Kaziga W, Afassinou YM, et al. Acute coronary syndromes: epidemiological, clinical, paraclinical and therapeutic characteristics at the Campus teaching hospital of Lome, Togo. Médecine Santé Trop 2018; 28(3): 285‑8.
Afassinou YM, Abdou S, Pessinaba S, Kaziga DD W, Atta B, et al. Management of Acute Coronary Syndromes in the Era of Interventional Cardiology in Togo. World J Cardiovasc Dis 2025; 15(5): 254-69.
Afassinou YM, Pessinaba S, Ehlan KE, Magoua NK, Borgatia A, Pio M, et al. From hypoglycemia to myocardial infarction: another particularity of diabetes. Sang Thromb Vaiss 2023; 35(1): 25‑7.
Afassinou Y, Edorh L, Pessinaba S, Atta B, Sodou A, Oloude N, et al. Spontaneous Dissection of the Coronary Artery: A Cause of Myocardial Infarction not to be forgotten in the Young Subject. Ann Vasc Med Res 2023; 10(1): 1‑4.
[12]
Grundy SM, Cleeman JI, Daniels SR, Donato KA, Eckel RH, Franklin BA, et al. Diagnosis and management of the metabolic syndrome: an American Heart Association/National Heart, Lung, and Blood Institute Scientific Statement. Circulation 2005; 112(17): 2735‑52.
Ryan T, Faxon D, Gunnar R, Kennedy J, King S, Loop F, et al. Guidelines for percutaneous transluminal coronary angioplasty. A report of the American College of Cardiology/American Heart Association Task Force on Assessment of Diagnostic and Therapeutic Cardiovascular Procedures (Subcommittee on Percutaneous Transluminal Coronary Angioplasty). Circulation 1988; 78(2): 486‑502.
Neumann FJ, Sousa-Uva M, Ahlsson A, Alfonso F, Banning AP, Benedetto U, et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. EuroIntervention J Eur Collab Work Group Interv Cardiol Eur Soc Cardiol 2019; 14(14): 1435‑534.
Yao H, Ekou A, Niamkey TJ, Soya EK, Aboley E, N’Guetta R. Coronary lesions in black African patients with acute coronary syndromes. Pan Afr Med J 2019; 32(104).
Schamroth C, ACCESS South Africa investigators. Management of acute coronary syndrome in South Africa: insights from the ACCESS (Acute Coronary Events - a Multinational Survey of Current Management Strategies) registry. Cardiovasc J Afr 2012; 23(7): 365‑70.
Isezuo S, Sani MU, Talle A, Johnson A, Adeoye AM, Ulgen MS, et al. Registry for Acute Coronary Events in Nigeria (RACE-Nigeria): Clinical Characterization, Management, and Outcome. J Am Heart Assoc 2022; 11(1): e020244.
Ticolat, P, Bertrand, E, Baeabe P, Bouramoue, C, Burdin, J, Diouf, S et al. Aspects épidémiologiques de la maladie coronaire chez le Noir Africain : à propos de 103 cas. Résultats de l’enquête multicentrique prospective CORONAFRIC. Cardiol Trop. 1991; 17: 7‑20.
[21]
Shavadia J, Yonga G, Otieno H. A prospective review of acute coronary syndromes in an urban hospital in sub-Saharan Africa. Cardiovasc J Afr 2012; 23(6): 318‑21.
Mignazonzon, A. Y., Soulemane, P., Saratou, A., Komlavi, Y., Dieu-donné, K. W., et al. (2025). Coronary Lesions and Myocardial Revascularisation in Acute Coronary Syndrome in Lome. Cardiology and Cardiovascular Research, 9(4), 113-119. https://doi.org/10.11648/j.ccr.20250904.11
Mignazonzon, A. Y.; Soulemane, P.; Saratou, A.; Komlavi, Y.; Dieu-donné, K. W., et al. Coronary Lesions and Myocardial Revascularisation in Acute Coronary Syndrome in Lome. Cardiol. Cardiovasc. Res.2025, 9(4), 113-119. doi: 10.11648/j.ccr.20250904.11
Mignazonzon AY, Soulemane P, Saratou A, Komlavi Y, Dieu-donné KW, et al. Coronary Lesions and Myocardial Revascularisation in Acute Coronary Syndrome in Lome. Cardiol Cardiovasc Res. 2025;9(4):113-119. doi: 10.11648/j.ccr.20250904.11
@article{10.11648/j.ccr.20250904.11,
author = {Afassinou Yaovi Mignazonzon and Pessinaba Soulemane and Abdou Saratou and Yayehd Komlavi and Kaziga Wiyaou Dieu-donné and Atta Borgatia and Sossou Yao Israël and Kpélafia Mohamed and Anifrani Déo and Pio Machihude and Baragou Soodougoua and Damorou Findibe},
title = {Coronary Lesions and Myocardial Revascularisation in Acute Coronary Syndrome in Lome
},
journal = {Cardiology and Cardiovascular Research},
volume = {9},
number = {4},
pages = {113-119},
doi = {10.11648/j.ccr.20250904.11},
url = {https://doi.org/10.11648/j.ccr.20250904.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ccr.20250904.11},
abstract = {Introduction and objective: Acute coronary syndrome (ACS) is a cardiac emergency, and significant progress has been made in its management in Togo. This study aimed to describe coronary lesions in ACS patients and aspects of myocardial revascularisation. Materials and methods: This cross-sectional study was conducted at Dogta-Lafiè Hospital and Autel d'Elie Private Hospital in Lomé over four years and six months (January 2021 to June 2025). All patients who underwent coronary angiography for acute coronary syndrome during the study period were included. Results: Out of 298 requests for coronary angiography for ACS, 184 patients underwent the procedure. The coronary angiography performance rate was 61.75%. The mean patient age was 57.9 ± 12.6 years, with a male predominance (sex ratio 1.8). ST-segment elevation myocardial infarction (STEMI) accounted for 62.5%. Significant coronary lesions were found in 161 patients (87.5%), which were significantly more prevalent in STEMI than in non-ST-segment elevation acute coronary syndrome (NSTE-ACS) (p = 0.0001). Depending on the complexity of the coronary lesions, type B lesions were significantly more prevalent in STEMI than in NSTE-ACS, while type C lesions were more prevalent in NSTE-ACS. Percutaneous coronary intervention was performed on only 86 patients (46.74% of those who underwent coronary angiography for ACS and 67.19% of those for whom percutaneous coronary intervention was indicated). Percutaneous coronary intervention was performed in 51 patients with STEMI (46.79%), including 13 cases of primary percutaneous coronary intervention (25.49%). Coronary artery bypass grafting was performed in 50% of patients for whom it was indicated. Two patients (1.56%) died from complications following angioplasty due to ventricular fibrillation. Conclusion: Coronary angiography is rarely performed in ACS, but it allows assessment of lesions. The rate of myocardial revascularisation also remains.
},
year = {2025}
}
TY - JOUR
T1 - Coronary Lesions and Myocardial Revascularisation in Acute Coronary Syndrome in Lome
AU - Afassinou Yaovi Mignazonzon
AU - Pessinaba Soulemane
AU - Abdou Saratou
AU - Yayehd Komlavi
AU - Kaziga Wiyaou Dieu-donné
AU - Atta Borgatia
AU - Sossou Yao Israël
AU - Kpélafia Mohamed
AU - Anifrani Déo
AU - Pio Machihude
AU - Baragou Soodougoua
AU - Damorou Findibe
Y1 - 2025/10/10
PY - 2025
N1 - https://doi.org/10.11648/j.ccr.20250904.11
DO - 10.11648/j.ccr.20250904.11
T2 - Cardiology and Cardiovascular Research
JF - Cardiology and Cardiovascular Research
JO - Cardiology and Cardiovascular Research
SP - 113
EP - 119
PB - Science Publishing Group
SN - 2578-8914
UR - https://doi.org/10.11648/j.ccr.20250904.11
AB - Introduction and objective: Acute coronary syndrome (ACS) is a cardiac emergency, and significant progress has been made in its management in Togo. This study aimed to describe coronary lesions in ACS patients and aspects of myocardial revascularisation. Materials and methods: This cross-sectional study was conducted at Dogta-Lafiè Hospital and Autel d'Elie Private Hospital in Lomé over four years and six months (January 2021 to June 2025). All patients who underwent coronary angiography for acute coronary syndrome during the study period were included. Results: Out of 298 requests for coronary angiography for ACS, 184 patients underwent the procedure. The coronary angiography performance rate was 61.75%. The mean patient age was 57.9 ± 12.6 years, with a male predominance (sex ratio 1.8). ST-segment elevation myocardial infarction (STEMI) accounted for 62.5%. Significant coronary lesions were found in 161 patients (87.5%), which were significantly more prevalent in STEMI than in non-ST-segment elevation acute coronary syndrome (NSTE-ACS) (p = 0.0001). Depending on the complexity of the coronary lesions, type B lesions were significantly more prevalent in STEMI than in NSTE-ACS, while type C lesions were more prevalent in NSTE-ACS. Percutaneous coronary intervention was performed on only 86 patients (46.74% of those who underwent coronary angiography for ACS and 67.19% of those for whom percutaneous coronary intervention was indicated). Percutaneous coronary intervention was performed in 51 patients with STEMI (46.79%), including 13 cases of primary percutaneous coronary intervention (25.49%). Coronary artery bypass grafting was performed in 50% of patients for whom it was indicated. Two patients (1.56%) died from complications following angioplasty due to ventricular fibrillation. Conclusion: Coronary angiography is rarely performed in ACS, but it allows assessment of lesions. The rate of myocardial revascularisation also remains.
VL - 9
IS - 4
ER -
Mignazonzon, A. Y., Soulemane, P., Saratou, A., Komlavi, Y., Dieu-donné, K. W., et al. (2025). Coronary Lesions and Myocardial Revascularisation in Acute Coronary Syndrome in Lome. Cardiology and Cardiovascular Research, 9(4), 113-119. https://doi.org/10.11648/j.ccr.20250904.11
Mignazonzon, A. Y.; Soulemane, P.; Saratou, A.; Komlavi, Y.; Dieu-donné, K. W., et al. Coronary Lesions and Myocardial Revascularisation in Acute Coronary Syndrome in Lome. Cardiol. Cardiovasc. Res.2025, 9(4), 113-119. doi: 10.11648/j.ccr.20250904.11
Mignazonzon AY, Soulemane P, Saratou A, Komlavi Y, Dieu-donné KW, et al. Coronary Lesions and Myocardial Revascularisation in Acute Coronary Syndrome in Lome. Cardiol Cardiovasc Res. 2025;9(4):113-119. doi: 10.11648/j.ccr.20250904.11
@article{10.11648/j.ccr.20250904.11,
author = {Afassinou Yaovi Mignazonzon and Pessinaba Soulemane and Abdou Saratou and Yayehd Komlavi and Kaziga Wiyaou Dieu-donné and Atta Borgatia and Sossou Yao Israël and Kpélafia Mohamed and Anifrani Déo and Pio Machihude and Baragou Soodougoua and Damorou Findibe},
title = {Coronary Lesions and Myocardial Revascularisation in Acute Coronary Syndrome in Lome
},
journal = {Cardiology and Cardiovascular Research},
volume = {9},
number = {4},
pages = {113-119},
doi = {10.11648/j.ccr.20250904.11},
url = {https://doi.org/10.11648/j.ccr.20250904.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ccr.20250904.11},
abstract = {Introduction and objective: Acute coronary syndrome (ACS) is a cardiac emergency, and significant progress has been made in its management in Togo. This study aimed to describe coronary lesions in ACS patients and aspects of myocardial revascularisation. Materials and methods: This cross-sectional study was conducted at Dogta-Lafiè Hospital and Autel d'Elie Private Hospital in Lomé over four years and six months (January 2021 to June 2025). All patients who underwent coronary angiography for acute coronary syndrome during the study period were included. Results: Out of 298 requests for coronary angiography for ACS, 184 patients underwent the procedure. The coronary angiography performance rate was 61.75%. The mean patient age was 57.9 ± 12.6 years, with a male predominance (sex ratio 1.8). ST-segment elevation myocardial infarction (STEMI) accounted for 62.5%. Significant coronary lesions were found in 161 patients (87.5%), which were significantly more prevalent in STEMI than in non-ST-segment elevation acute coronary syndrome (NSTE-ACS) (p = 0.0001). Depending on the complexity of the coronary lesions, type B lesions were significantly more prevalent in STEMI than in NSTE-ACS, while type C lesions were more prevalent in NSTE-ACS. Percutaneous coronary intervention was performed on only 86 patients (46.74% of those who underwent coronary angiography for ACS and 67.19% of those for whom percutaneous coronary intervention was indicated). Percutaneous coronary intervention was performed in 51 patients with STEMI (46.79%), including 13 cases of primary percutaneous coronary intervention (25.49%). Coronary artery bypass grafting was performed in 50% of patients for whom it was indicated. Two patients (1.56%) died from complications following angioplasty due to ventricular fibrillation. Conclusion: Coronary angiography is rarely performed in ACS, but it allows assessment of lesions. The rate of myocardial revascularisation also remains.
},
year = {2025}
}
TY - JOUR
T1 - Coronary Lesions and Myocardial Revascularisation in Acute Coronary Syndrome in Lome
AU - Afassinou Yaovi Mignazonzon
AU - Pessinaba Soulemane
AU - Abdou Saratou
AU - Yayehd Komlavi
AU - Kaziga Wiyaou Dieu-donné
AU - Atta Borgatia
AU - Sossou Yao Israël
AU - Kpélafia Mohamed
AU - Anifrani Déo
AU - Pio Machihude
AU - Baragou Soodougoua
AU - Damorou Findibe
Y1 - 2025/10/10
PY - 2025
N1 - https://doi.org/10.11648/j.ccr.20250904.11
DO - 10.11648/j.ccr.20250904.11
T2 - Cardiology and Cardiovascular Research
JF - Cardiology and Cardiovascular Research
JO - Cardiology and Cardiovascular Research
SP - 113
EP - 119
PB - Science Publishing Group
SN - 2578-8914
UR - https://doi.org/10.11648/j.ccr.20250904.11
AB - Introduction and objective: Acute coronary syndrome (ACS) is a cardiac emergency, and significant progress has been made in its management in Togo. This study aimed to describe coronary lesions in ACS patients and aspects of myocardial revascularisation. Materials and methods: This cross-sectional study was conducted at Dogta-Lafiè Hospital and Autel d'Elie Private Hospital in Lomé over four years and six months (January 2021 to June 2025). All patients who underwent coronary angiography for acute coronary syndrome during the study period were included. Results: Out of 298 requests for coronary angiography for ACS, 184 patients underwent the procedure. The coronary angiography performance rate was 61.75%. The mean patient age was 57.9 ± 12.6 years, with a male predominance (sex ratio 1.8). ST-segment elevation myocardial infarction (STEMI) accounted for 62.5%. Significant coronary lesions were found in 161 patients (87.5%), which were significantly more prevalent in STEMI than in non-ST-segment elevation acute coronary syndrome (NSTE-ACS) (p = 0.0001). Depending on the complexity of the coronary lesions, type B lesions were significantly more prevalent in STEMI than in NSTE-ACS, while type C lesions were more prevalent in NSTE-ACS. Percutaneous coronary intervention was performed on only 86 patients (46.74% of those who underwent coronary angiography for ACS and 67.19% of those for whom percutaneous coronary intervention was indicated). Percutaneous coronary intervention was performed in 51 patients with STEMI (46.79%), including 13 cases of primary percutaneous coronary intervention (25.49%). Coronary artery bypass grafting was performed in 50% of patients for whom it was indicated. Two patients (1.56%) died from complications following angioplasty due to ventricular fibrillation. Conclusion: Coronary angiography is rarely performed in ACS, but it allows assessment of lesions. The rate of myocardial revascularisation also remains.
VL - 9
IS - 4
ER -