Chronic Obstructive Pulmonary Disease (COPD) is a common comorbidity in patients with aortic stenosis and when severe is a surgical aortic valve replacement contraindication. However, the impact of COPD in patients undergoing TAVR is unclear. This study defines TAVR risks/benefits including quality of life, morbidities, and mortality in COPD patients. All patients undergoing TAVR from August 2012 to June 2023 at a single institution were retrospectively reviewed (n = 1565). 1273 patients with preoperative pulmonary function testing were studied. FEV1/FVC and FEV1% predicted were used to separate patients into groups of COPD severity based on the GOLD (Global Initiative for Chronic Obstructive Lung Disease) criteria. Preoperative and postoperative quality of life (QoL) were measured with the Kansas City Cardiomyopathy Questionnaire (KCCQ). Adverse outcomes and mortality at 30-days and 1-year were measured. Severe and very severe COPD patients had significantly higher rates of new onset atrial fibrillation and myocardial infarction compared to patients with no COPD or mild to moderate COPD. There were no statistically significant differences in rates of stroke, permanent pacemaker implantation, 30-day mortality, or 1-year mortality. TAVR improved QoL in all patients regardless of COPD severity or use of home oxygen. Severe COPD patients had the greatest improvement in KCCQ QoL at 30-days and 1-year post-TAVR, while very severe COPD patients had the smallest improvement in KCCQ QoL. Patients with COPD experienced an improvement in quality of life regardless of severity of COPD. Additionally, one year mortality was not significantly different between COPD severity groups. Therefore, TAVR benefits should not be withheld for COPD patients regardless of their severity.
| Published in | Cardiology and Cardiovascular Research (Volume 8, Issue 4) |
| DOI | 10.11648/j.ccr.20240804.13 |
| Page(s) | 104-112 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Structural Heart Disease, Transcatheter Aortic Valve Replacement (TAVR), Chronic Obstructive Pulmonary Disease (COPD)
GOLD Class | Criteria |
|---|---|
Mild | FEV1/FVC < 0.7 and FEV1% predicted ≥ 80% |
Moderate | FEV1/FVC < 0.7 and 50% ≤ FEV1% predicted < 80% |
Severe | FEV1/FVC < 0.7 and 30% ≤ FEV1% predicted < 50% |
Very Severe | FEV1/FVC < 0.7 and FEV1% predicted < 30% |
Demographic | All Patients |
|---|---|
STS Score | 18.45 |
Gender (% F) | 42.30% |
BMI | 30.42 |
Age at Procedure | 79 |
Tobacco Use History | 58.66% |
Smoking History | 57.57% |
Diabetes | 35.14% |
HTN | 85.75% |
CAD | 67.92% |
CHF | 40.64% |
PVD | 12.74% |
CKD | 27.80% |
Hyperlipidemia | 77.32% |
Hypercholesterolemia | 20.77% |
Stroke/TIA | 12.52% |
Demographic | None | Mild | Moderate | Severe | Very Severe | p-value |
|---|---|---|---|---|---|---|
STS Score | 17.73 | 27.43 | 26.43 | 5.00 | 4.72 | <0.0001 |
Gender (% F) | 45.93% | 32.73% | 33.67% | 29.89% | 29.41% | 0.0003 |
BMI | 31.40 | 28.34 | 30.28 | 29.35 | 27.09 | <0.0001 |
Age at Procedure | 78.44 | 81.78 | 78.60 | 74.90 | 73.13 | <0.0001 |
Tobacco Use History | 51.16% | 65.45% | 79.08% | 83.91% | 82.35% | <0.0001 |
Smoking History | 50.12% | 62.73% | 78.57% | 83.91% | 82.35% | <0.0001 |
Diabetes | 38.49% | 20.91% | 36.22% | 29.89% | 11.76% | 0.0008 |
HTN | 87.33% | 80.91% | 84.10% | 83.91% | 70.59% | 0.1010 |
CAD | 67.91% | 66.36% | 63.78% | 67.82% | 58.82% | 0.7721 |
CHF | 35.81% | 33.64% | 46.43% | 58.62% | 47.06% | <0.0001 |
PVD | 10.81% | 12.73% | 13.78% | 18.39% | 5.88% | 0.2158 |
CKD | 28.37% | 19.09% | 26.53% | 28.74% | 11.76% | 0.2836 |
Hyperlipidemia | 81.63% | 75.45% | 76.53% | 74.71% | 64.71% | 0.0886 |
Hypercholesterolemia | 23.05% | 16.36% | 16.33% | 20.69% | 11.76% | 0.1348 |
Clinical Outcomes | All Patients (n = 1273) | None (n = 861) | Mild (n = 110) | Moderate (n = 198) | Severe (n = 87) | Very Severe (n = 17) | p-value |
|---|---|---|---|---|---|---|---|
Stroke | 68 (5.34%) | 48 (5.57%) | 4 (3.64%) | 12 (6.06%) | 4 (4.60%) | 0 (0.00%) | 0.6969 |
TIA or Delirium | 38 (2.99%) | 22 (2.56%) | 5 (4.55%) | 6 (3.03%) | 5 (5.75%) | 0 (0.00%) | |
Pacemaker | 150 (11.78%) | 103 (11.96%) | 12 (10.91%) | 22 (11.11%) | 11 (12.64%) | 2 (11.76%) | 0.9898 |
New Onset Atrial fibrillation | 172 (13.51%) | 106 (12.31%) | 15 (13.64%) | 24 (12.12%) | 21 (24.14%) | 6 (35.29%) | 0.0046 |
MI | 219 (17.20%) | 138 (16.03%) | 15 (13.64%) | 37 (18.69%) | 25 (28.74%) | 4 (23.53%) | 0.0342 |
30-Day Mortality Rate | 41 (3.22%) | 27 (3.14%) | 6 (5.45%) | 7 (3.54%) | 1 (1.15%) | 0 (0.00%) | 0.5281 |
1-Year Mortality Rate | 131 (10.29%) | 78 (9.06%) | 17 (15.45%) | 24 (12.12%) | 9 (10.34%) | 3 (17.65%) | 0.1369 |
Clinical Outcome | All (n =1561) | No Home Oxygen (n = 1422) | Home Oxygen (n = 139) | p-value |
|---|---|---|---|---|
Stroke | 85 (5.45 %) | 72 (5.06%) | 13 (9.35%) | 0.0156 |
TIA or Delirium | 49 (3.14%) | 41 (2.88%) | 8 (5.76%) | |
Pacemaker | 177 (11.34%) | 156 (10.97%) | 21 (15.11%) | 0.1420 |
New Onset Atrial fibrillation | 198 (12.68%) | 183 (12.87%) | 15 (10.79%) | 0.5929 |
MI | 254 (16.27%) | 221 (15.54%) | 33 (23.74%) | 0.0158 |
30-Day Mortality Rate | 51 (3.27%) | 47 (3.31%) | 4 (2.88%) | 1.0000 |
1-Year Mortality Rate | 165 (10.57%) | 142 (9.99%) | 23 (16.55%) | 0.0163 |
KCCQ Time | None | Mild | Moderate | Severe | Very Severe | p-value |
|---|---|---|---|---|---|---|
Preoperative | 40.85 (32 – 49) | 41.19 (34 – 48) | 36.53 (29 – 44) | 33.22 (24 – 40) | 34.44 (28 – 41.5) | <.0001 |
(n = 833) | (n = 109) | (n = 190) | (n = 85) | (n = 16) | ||
30-Days | 58.31 (55 – 64) | 56.19 (51 – 64) | 55.95 (51 – 64) | 53.47 (49 – 62) | 50.33 (41 – 60) | <.0001 |
(n = 761) | (n = 95) | (n = 171) | (n = 77) | (n = 15) | ||
1-Year | 59.25 (58 – 64) | 57.2 (53 – 64) | 57.09 (54 – 64) | 55.12 (48 – 64) | 50.57 (42 – 61) | <.0001 |
(n = 587) | (n = 65) | (n = 137) | (n = 58) | (n = 7) | ||
Change at 30-Days | 17.16 (9 – 26) | 14.74 (6 – 23) | 18.80 (11 – 28) | 19.99 (11 – 29) | 14.47 (5 – 25) | 0.0097 |
(n = 752) | (n = 95) | (n = 171) | (n = 77) | (n = 15) | ||
Change at 1-Year | 17.86 (9 – 27) | 16.27 (8 – 24) | 20.89 (11 – 31) | 20.79 (12 – 29) | 13 (4 – 16) | 0.0166 |
(n = 573) | (n = 64) | (n = 133) | (n = 56) | (n = 7) |
KCCQ Time | No Home Oxygen | Home Oxygen | p-value |
|---|---|---|---|
Preoperative | 40.14 (31 – 48) | 31.70 (25 – 38) | <.0001 |
(n = 1380) | (n = 132) | ||
30-Days | 57.97 (55 – 64) | 52.28 (47 – 62) | <.0001 |
(n = 1250) | (n = 113) | ||
1-Year | 59.09 (57 – 64) | 53.53 (47 – 62) | <.0001 |
(n = 935) | (n = 83) | ||
Change at 30-Days | 17.56 (9 – 26) | 20.31 (12 – 29.5) | 0.0223 |
(n = 1238) | (n = 112) | ||
Change at 1-Year | 18.59 (10 – 28) | 21.28 (12 – 30) | 0.0650 |
(n = 910) | (n = 82) |
COPD | Chronic Obstructive Pulmonary Disease |
TAVR | Transcatheter Aortic Valve Replacement |
QoL | Quality of Life |
KCCQ | Kansas City Cardiomyopathy Questionnaire |
SAVR | Surgical Aortic Valve Replacement |
GOLD | Global Initiative for Chronic Obstructive Lung Disease |
FEV1 | Forced Expiratory Volume in 1 Second |
FVC | Forced Vital Capacity |
FEV1% | Forced Expiratory Volume in 1 Second Percentage of the Predicted Value |
VARC | Valve Academic Research Consortium 3 |
STS | Society of Thoracic Surgery |
BMI | Body Mass Index |
HTN | Hypertension |
CAD | Coronary Artery Disease |
CHF | Congestive Heart Failure |
PVD | Peripheral Vascular Disease |
CKD | Chronic Kidney Disease |
TIA | Transient Ischemic Attack |
MI | Myocardial Infarction |
HmO2 | Home Oxygen |
| [1] | Lauridsen MD, Valentin JB, Strange JE, et al. Mortality in patients with chronic obstructive pulmonary disorder undergoing transcatheter aortic valve replacement: The importance of chronic obstructive pulmonary disease exacerbation. American Heart Journal. 2023; 262: 100-109. |
| [2] | Tamburino C, Capodanno D, Ramondo A, et al. Incidence and predictors of early and late mortality after transcatheter aortic valve implantation in 663 patients with severe aortic stenosis. Circulation. 2011; 123(3): 299-308. |
| [3] | Mok M, Nombela-Franco L, Dumont E, et al. Chronic Obstructive Pulmonary Disease in Patients Undergoing Transcatheter Aortic Valve Implantation: Insights on Clinical Outcomes, Prognostic Markers, and Functional Status Changes. JACC: Cardiovascular Interventions. 2013; 6(10): 1072-1084. |
| [4] | Ando T, Adegbala O, Akintoye E, et al. Is Transcatheter Aortic Valve Replacement Better Than Surgical Aortic Valve Replacement in Patients With Chronic Obstructive Pulmonary Disease? A Nationwide Inpatient Sample Analysis. Journal of the American Heart Association. 2018; 7(7): e008408. |
| [5] | Kwak MJ, Bhise V, Warner MT, et al. National trend of utilization, clinical and economic outcomes of transcatheter aortic valve replacement among patients with chronic obstructive pulmonary disease. Curr Med Res Opin. 2019; 35(8): 1321-1329. |
| [6] | Nuche J, Ternacle J, Avvedimento M, et al. Incidence, predictors, and prognostic significance of impaired functional status early after transcatheter aortic valve replacement. Rev Esp Cardiol (Engl Ed). 2024; 77(5): 396-407. |
| [7] | Xiao F, Yang J, Fan R. Effects of COPD on in-hospital outcomes of transcatheter aortic valve implantation: Results from the National Inpatient Sample database. Clin Cardiol. 2020; 43(12): 1524-1533. |
| [8] | Doldi P, Steffen J, Orban M, et al. Clinical Outcome Following Transcatheter Aortic Valve Implantation in Patients With Chronic Obstructive Pulmonary Disease. JACC: Cardiovascular Interventions. 2022; 15(11): 1188-1190. |
| [9] | Dziewierz A, Tokarek T, Kleczynski P, et al. Impact of chronic obstructive pulmonary disease and frailty on long-term outcomes and quality of life after transcatheter aortic valve implantation. Aging Clin Exp Res. 2018; 30(9): 1033-1040. |
| [10] | Mach M, Koschutnik M, Wilbring M, et al. Impact of COPD on Outcome in Patients Undergoing Transfemoral versus Transapical TAVI. Thorac Cardiovasc Surg. 2019; 67(4): 251-256. |
| [11] | Marzec K, Jaworska-Wilczyńska M, Kowalik I, et al. Comparison of long-term outcomes and risk factors of aortic stenosis treatment in patients undergoing transcatheter aortic valve implantation and surgical aortic valve replacement. Kardiol Pol. 2022; 80(7-8): 792-798. |
| [12] | Myagmardorj R, Nabeta T, Hirasawa K, et al. Association Between Chronic Obstructive Pulmonary Disease and All-Cause Mortality After Aortic Valve Replacement for Aortic Stenosis. Am J Cardiol. 2023; 190: 41-47. |
| [13] | Dvir D, Waksman R, Barbash IM, et al. Outcomes of Patients With Chronic Lung Disease and Severe Aortic Stenosis Treated With Transcatheter Versus Surgical Aortic Valve Replacement or Standard Therapy. Journal of the American College of Cardiology. 2014; 63(3): 269-279. |
| [14] | Patail H, Kompella R, Hoover NE, et al. In-Hospital and One-Year Outcomes of Transcatheter Aortic Valve Replacement in Patients Requiring Supplemental Home Oxygen Use. Cardiol Res. 2023; 14(3): 228-236. |
| [15] | Agustí A, Celli BR, Criner GJ, et al. Global Initiative for Chronic Obstructive Lung Disease 2023 Report: GOLD Executive Summary. Eur Respir J. 2023; 61(4): 2300239. |
| [16] | Généreux P, Piazza N, Alu MC, et al. Valve Academic Research Consortium 3: Updated Endpoint Definitions for Aortic Valve Clinical Research. Journal of the American College of Cardiology. 2021; 77(21): 2717-2746. |
| [17] | Arnold SV, Spertus JA, Vemulapalli S, et al. Quality of Life Outcomes after Transcatheter Aortic Valve Replacement in an Unselected Population. A Report from the STS/ACC TVT Registry™. JAMA Cardiol. 2017; 2(4): 409-416. |
APA Style
Schwartz, G., Row, H., Tupa, J., Matter, A., Sahmoun, A., et al. (2024). Transcatheter Aortic Valve Replacement Improves the Quality of Life for Patients with Chronic Obstructive Pulmonary Disease. Cardiology and Cardiovascular Research, 8(4), 104-112. https://doi.org/10.11648/j.ccr.20240804.13
ACS Style
Schwartz, G.; Row, H.; Tupa, J.; Matter, A.; Sahmoun, A., et al. Transcatheter Aortic Valve Replacement Improves the Quality of Life for Patients with Chronic Obstructive Pulmonary Disease. Cardiol. Cardiovasc. Res. 2024, 8(4), 104-112. doi: 10.11648/j.ccr.20240804.13
AMA Style
Schwartz G, Row H, Tupa J, Matter A, Sahmoun A, et al. Transcatheter Aortic Valve Replacement Improves the Quality of Life for Patients with Chronic Obstructive Pulmonary Disease. Cardiol Cardiovasc Res. 2024;8(4):104-112. doi: 10.11648/j.ccr.20240804.13
@article{10.11648/j.ccr.20240804.13,
author = {Greta Schwartz and Hunter Row and Jacob Tupa and Ashley Matter and Abe Sahmoun and Thomas Haldis and Cornelius Dyke},
title = {Transcatheter Aortic Valve Replacement Improves the Quality of Life for Patients with Chronic Obstructive Pulmonary Disease
},
journal = {Cardiology and Cardiovascular Research},
volume = {8},
number = {4},
pages = {104-112},
doi = {10.11648/j.ccr.20240804.13},
url = {https://doi.org/10.11648/j.ccr.20240804.13},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ccr.20240804.13},
abstract = {Chronic Obstructive Pulmonary Disease (COPD) is a common comorbidity in patients with aortic stenosis and when severe is a surgical aortic valve replacement contraindication. However, the impact of COPD in patients undergoing TAVR is unclear. This study defines TAVR risks/benefits including quality of life, morbidities, and mortality in COPD patients. All patients undergoing TAVR from August 2012 to June 2023 at a single institution were retrospectively reviewed (n = 1565). 1273 patients with preoperative pulmonary function testing were studied. FEV1/FVC and FEV1% predicted were used to separate patients into groups of COPD severity based on the GOLD (Global Initiative for Chronic Obstructive Lung Disease) criteria. Preoperative and postoperative quality of life (QoL) were measured with the Kansas City Cardiomyopathy Questionnaire (KCCQ). Adverse outcomes and mortality at 30-days and 1-year were measured. Severe and very severe COPD patients had significantly higher rates of new onset atrial fibrillation and myocardial infarction compared to patients with no COPD or mild to moderate COPD. There were no statistically significant differences in rates of stroke, permanent pacemaker implantation, 30-day mortality, or 1-year mortality. TAVR improved QoL in all patients regardless of COPD severity or use of home oxygen. Severe COPD patients had the greatest improvement in KCCQ QoL at 30-days and 1-year post-TAVR, while very severe COPD patients had the smallest improvement in KCCQ QoL. Patients with COPD experienced an improvement in quality of life regardless of severity of COPD. Additionally, one year mortality was not significantly different between COPD severity groups. Therefore, TAVR benefits should not be withheld for COPD patients regardless of their severity.
},
year = {2024}
}
TY - JOUR T1 - Transcatheter Aortic Valve Replacement Improves the Quality of Life for Patients with Chronic Obstructive Pulmonary Disease AU - Greta Schwartz AU - Hunter Row AU - Jacob Tupa AU - Ashley Matter AU - Abe Sahmoun AU - Thomas Haldis AU - Cornelius Dyke Y1 - 2024/12/13 PY - 2024 N1 - https://doi.org/10.11648/j.ccr.20240804.13 DO - 10.11648/j.ccr.20240804.13 T2 - Cardiology and Cardiovascular Research JF - Cardiology and Cardiovascular Research JO - Cardiology and Cardiovascular Research SP - 104 EP - 112 PB - Science Publishing Group SN - 2578-8914 UR - https://doi.org/10.11648/j.ccr.20240804.13 AB - Chronic Obstructive Pulmonary Disease (COPD) is a common comorbidity in patients with aortic stenosis and when severe is a surgical aortic valve replacement contraindication. However, the impact of COPD in patients undergoing TAVR is unclear. This study defines TAVR risks/benefits including quality of life, morbidities, and mortality in COPD patients. All patients undergoing TAVR from August 2012 to June 2023 at a single institution were retrospectively reviewed (n = 1565). 1273 patients with preoperative pulmonary function testing were studied. FEV1/FVC and FEV1% predicted were used to separate patients into groups of COPD severity based on the GOLD (Global Initiative for Chronic Obstructive Lung Disease) criteria. Preoperative and postoperative quality of life (QoL) were measured with the Kansas City Cardiomyopathy Questionnaire (KCCQ). Adverse outcomes and mortality at 30-days and 1-year were measured. Severe and very severe COPD patients had significantly higher rates of new onset atrial fibrillation and myocardial infarction compared to patients with no COPD or mild to moderate COPD. There were no statistically significant differences in rates of stroke, permanent pacemaker implantation, 30-day mortality, or 1-year mortality. TAVR improved QoL in all patients regardless of COPD severity or use of home oxygen. Severe COPD patients had the greatest improvement in KCCQ QoL at 30-days and 1-year post-TAVR, while very severe COPD patients had the smallest improvement in KCCQ QoL. Patients with COPD experienced an improvement in quality of life regardless of severity of COPD. Additionally, one year mortality was not significantly different between COPD severity groups. Therefore, TAVR benefits should not be withheld for COPD patients regardless of their severity. VL - 8 IS - 4 ER -
Department of Surgery, University of North Dakota School of Medicine and Health Sciences, Grand Forks, United States
Research Fields: Transcatheter Aortic Valve Replacement, Cardiology, Rural Medicine, Biomedical Engineering, Cardiovascular Health Disparities
Department of Surgery, University of North Dakota School of Medicine and Health Sciences, Grand Forks, United States
Research Fields: Transcatheter Aortic Valve Replacement, Cardiovascular Surgery, Cardiac Surgical Outcomes, Hemostasis and Coagulation, Cardiovascular Health Disparities
Department of Surgery, University of North Dakota School of Medicine and Health Sciences, Grand Forks, United States
Research Fields: Transcatheter Aortic Valve Replacement, Cardiothoracic Surgery, Rural Health Disparities, ENT Conditions, Head & Neck surgery
Department of Surgery, University of North Dakota School of Medicine and Health Sciences, Grand Forks, United States
Research Fields: Transcatheter Aortic Valve Replacement, Orthopedic Surgery, Cardiology, General Surgery, Cardiothoracic Surgery
Department of Surgery, University of North Dakota School of Medicine and Health Sciences, Grand Forks, United States
Research Fields: Epidemiology, Biostatistics, Health Services Research, Oncology, Surgery, Quality of care
Department of Cardiology, Sanford Health, Fargo, United States
Research Fields: Transcatheter Aortic Valve Replacement, Interventional Cardiology, Vascular Medicine, Endovascular Interventions, Cardiovascular Health Disparities
Department of Surgery, University of North Dakota School of Medicine and Health Sciences, Grand Forks, United States;Department of Cardiothoracic Surgery, Sanford Health, Fargo, United States
Research Fields: Cardiovascular Health Disparities, Cardiac Surgical Outcomes, Patient Blood Management, Hemostasis and Coagulation, Perioperative Blood Pressure Management
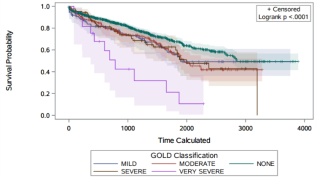
Figure 1. Graph showing the survival probability of each GOLD COPD severity group as a function of time (days) following TAVR over about 7 years.
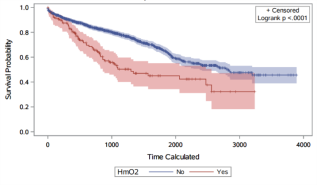
Figure 2. Graph showing the survival probability of the home oxygen group compared to the non-home oxygen group as a function of time (days) following TAVR over about 7 years.

