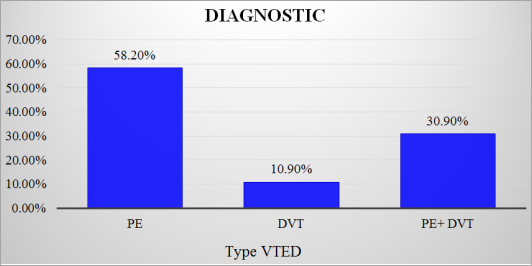
Introduction: Venous thromboembolic diseases (VTED) include deep vein thrombosis of the lower limbs and pulmonary embolism (PE), which is its severe form due to its high mortality. The objective of our study was to determine the epidemio-clinical and paraclinical aspects of patients hospitalized for venous thromboembolic diseases. Patients and method: Cross-sectional study with prospective recruitment from patient records hospitalized for (VTED) from January to December 2023 in the cardiology department of the Mother-Child University Hospital in Bamako, Luxembourg. Results: We collected 55 out of 580 patient records hospitalized for (VTED), a hospital frequency of 9.48%. PE accounted for 58.20% of cases, 10.90% for deep vein thrombosis (DVT), and 30.90% for their association. The mean age of patients was 55.56 years ± 15.52 years. The majority of patients, 90%, were under 66 years of age. The predominance was female, 56%. In lower extremity DVT, calf pain and Homans' sign were present in 56% and 24% of patients. In pulmonary embolism, dyspnea and chest pain were present in 85.50% and 65.50% of patients. Etiological factors were dominated by neoplasia in 10.90%, contraception 5.45% and orthopedic surgery in 5.45% of cases. Cardiovascular risk factors were a sedentary lifestyle (50.90%), obesity (34.45%), high blood pressure (36.36%) and diabetes (21.81%). Laboratory abnormalities were elevation of troponin (46.87%), BNP (40.62%), D-Dimer (62.50%) and anemia (9.09%). Electrocardiographic abnormalities were tachycardia in 65.4% and S1Q3 in 21.81% of patients. Echocardiography showed dilation of the right cavities (47.27%), systolic pulmonary arterial hypertension (38.18%) and thrombus in the right cavitary (5.45%). On thoracic CT angiography, PE was proximal (36.40%), bilateral (61.80%) and massive (29.10%). On venous Doppler ultrasound, TVP was proximal in 65.21%. Conclusion: VETD was more common in women and younger subjects.
| Published in | Cardiology and Cardiovascular Research (Volume 8, Issue 2) |
| DOI | 10.11648/j.ccr.20240802.14 |
| Page(s) | 73-77 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Thromboembolic Diseases, Epidemiology, Clinical, Paraclinical, Mali
CV risk factor and Etiological Factors | Number | % |
|---|---|---|
High blood pressure | 20 | 36,36 |
Diabetes | 12 | 21,81 |
Dyslipidemia | 4 | 7,27 |
TOBACCO | 7 | 12,72 |
Obesity | 19 | 34,45 |
Sedentary lifestyle | 28 | 50,90 |
History of DVT | 2 | 3,63 |
History of PE | 4 | 7,27 |
CANCER | 6 | 10,90 |
Pregnancy or postpartum | 2 | 3,63 |
Contraception | 3 | 5,45 |
Orthopedic surgery | 3 | 5,45 |
Table II: Paraclinical data |
Para-clinical data | Number | % | |
|---|---|---|---|
Biology n = 32 | D-Dimer | 20 | 62,50 |
Troponins | 15 | 46,87 | |
NPP | 13 | 40,62 | |
ECG n=55 | Tachycardia | 36 | 65,45 |
S1Q3 | 12 | 21,81 | |
BBD | 3 | 5,45 | |
FA | 1 | 1,81 | |
Negative T Waves V1-V4 | 4 | 7,27 | |
Cardiac Doppler Echo n= 55 | Right-hand cavity expansion | 26 | 47,27 |
PAH | 21 | 38,18 | |
Intracavitary thrombus | 3 | 5,45 | |
VCI Expansion | 6 | 10,90 | |
Venous Doppler ultrasound n=23 | Proximal DVT | 15 | 65,21 |
Distal DVT | 8 | 34,78 | |
CT angiography of pulmonary arteries n= 30 | Proximal PE | 17 | 56,66 |
Distal PE | 19 | 43,33 | |
Unilateral PE | 11 | 36,66 | |
Bilateral PE | 19 | 63,33 | |
Massive PE | 8 | 26,66 | |
VTED | Venous Thromboembolic Disease |
PE | Pulmonary Embolism |
DVT | Deep Vein Thrombosis |
PAH | Pulmonary Arterial Hypertension |
BNP | Brun Natriuretic Peptide |
MI | Lower Extremities |
BBD | Right Branch Block |
IVC | Inferior Vena Cava |
| [1] | Godier A., Lakhdari M., Samama C. M. – Maladie thromboembolique veineuse en réanimation. [Venous thromboembolic disease in intensive care]. Conférence d’actualisation. 53e congrès national d’anesthésie réanimation SFAR 2001. |
| [2] | Emmerich J. – Fréquence et facteurs de risque de la maladie veineuse thromboembolique [Frequency and risk factors for throm-boembolic venous disease]. La Revue du Praticien 2003; 53, 1: 14-19. |
| [3] | Cohen AT, Agnelli G, Anderson FA, et al. Venous thromboembo lism (VTE) in Europe. The number of VTE events and associated morbidity and mortality. Thromb Haemost 2007; 98: 756-64. |
| [4] | Findibe Damorou, Soodougoua Baragou, Machihuede Pio, Yaovi M Afassinou, N'kenon W N'da, Soulemane Pessinaba, Tchaa Tchérou, Halé Attiogbé, Koffi Ehlan, Edem Goeh-Akue, et Komlavi Yayehd. Morbidité et mortalité hospitalière des maladies cardiovasculaires en milieu tropical: exemple d'un centre hospitalier à Lomé (Togo). [Hospital morbidity and mortality of cardiovascular diseases in tropical environments: example of a hospital in Lomé (Togo)]. Pan Afr Med J 2014; 17: 62. Publication en ligne 2014 janv. 26. French. |
| [5] | Owono Etoundi P, Esiéne A, Bengono Bengono R, Amengle L, Afane Ela A, Ze Minkande J. La Maladie Thromboembolique Veineuse. Aspects Épidémiologiques et Facteurs de Risque dans un Hôpital Camerounais. [Venous thromboembolic disease. Epidemiological Aspects and Risk Factors in a Cameroonian Hospital] Health Sci. Dis 2015; 16 (4): 1-4. |
| [6] | Igun G. A 10-year review of venous thrombo-embolism in surgical patients seen in Jos, Nigeria. Niger Prostgrad Med J 2001; 8(2): 69-73. |
| [7] | Coulibaly S, Menta I, Diall IB, Ba HO, Diakité M, Sidibé S, Diallo N, Kodio A, Traoré S, Kané K, Sidibé S, Touré K, Camara Y, Konaté M, Kéita A, Thiam CA, Diallo B. Maladie thromboembolique veineuse dans un-CHU de Bamako. [Venous thromboembolic disease in a University Hospital in Bamako] Health Sci. Dis: Vol 19 (2) April – May – June 2018 Available at |
| [8] | Thiam A., Tindano C., Kologo J., Millogo GR., Yaméogo NV., Kagambega LJ., Samadoulougou AK., Zabsonré P. Maladie thromboembolique veineuse au Burkina Faso. Résultats préliminaires du registre prospectif REMAVET. [Preliminary results of the REMAVET prospective register]. Livre des résumés des 5èmes journées scientifiques de la SOCARB 2015. |
| [9] | Mbaye A., Dioum M., Ngaïdé AA., Diop A., Leye M. C. B. O., Ka M. M., Kouamé I., Ndiaye M., Cissé AF., Dieng M., Faye MO., Dia S., Babaka K., Aw F., SA. S: La maladie thrombo-embolique veineuse: prévalence, facteurs étiologiques et prise en charge en service de cardiologie à Dakar au Sénégal. [Venous thromboembolic disease: prevalence, etiological factors and management in the cardiology department in Dakar, Senegal.] Angéiologie 2016; 68(3): 47-53. |
| [10] | Nourelhouda C, Abbassia D. Maladie thromboembolique veineuse dans la région de Sidi Bel Abbes, Algérie: fréquence et facteurs de risque. [Venous thromboembolic disease in the Sidi Bel Abbes region, Algeria: frequency and risk factors] Pan Afr Med J 2013; 16: 45. Publication en ligne 2013 oct. 10. French. |
| [11] | Simeni Njonnou. S. R, Nganou Gnindjio. C. N, Ba. H, Boombhi. J, Ahmadou Musa. J, Kuate. M. L, Pefura. Y. E. W, Menanga. A. P, Kingue. S: Épidémiologie de le maladie veineuse thromboembolique à Yaoundé: étude transversale en Afrique subsaharienne. [Epidemiology of thromboembolic venous disease in Yaoundé: a cross-sectional study in sub-Saharan Africa] La Revue de Médecine Interne 2019; 40 (supp 1): A186.10. |
| [12] | Camara Y, Bâ HO, Sangaré I, Sidibé N, Thiam ep Doumbia C, Keita ep Maiga A. et al, Maladie thromboembolique: aspects épidémio-cliniques et thérapeutiques au CHU de Kati. [Thromboembolic disease: epidemio-clinical and therapeutic aspects at the Kati University Hospital] Health Sci. Dis: Vol 22 (4) April 2022 pp 86-89 Available free at |
| [13] | Ondze-Kafata L. I., Kouala Landa C., Traore Kissima A., Loumouamou M., Bani M., Amounya Zobo S. et al – La thrombose veineuse des membres inférieurs à brazzaville: à propos de 44 cas. [Venous thrombosis of the lower limbs in Brazzaville: about 44 cases] Cardiologie Tropicale 2012; 135. |
| [14] | Diall I. B., Coulibaly S., Minta I., Ba Ho, Diakite M., Sidibe N. et al. – Etiologie, clinique et évolution de l’embolie pulmonaire. A propos de 30 cas. [Etiology, clinic and evolution of pulmonary embolism. About 30 cases] Mali Médical 2011; 26, 1: 3-6. |
| [15] | Diedhiou D., Sarr A., Ndour-Mbaye N. M., Ka Cisse M., Diop S. N. – Phlébite des membres inférieurs en médecine interne. Aspects épidémiologiques, cliniques et étiologiques. A propos de 40 cas dakarois [Phlebitis of the lower limbs in internal medicine. Epidemiological, clinical and etiological aspects. About 40 Dakar cases]. Médecine Afrique Noire 2012; 59, 3: 172-176. |
APA Style
Mamadou, T., Adiaratou, T. C., Daouda, F., Hamma, S., Mariam, D., et al. (2024). Epidemio-Clinical and Paraclinical Aspects of Venous Thromboembolic Diseases in a Cardiology Department in Mali. Cardiology and Cardiovascular Research, 8(2), 73-77. https://doi.org/10.11648/j.ccr.20240802.14
ACS Style
Mamadou, T.; Adiaratou, T. C.; Daouda, F.; Hamma, S.; Mariam, D., et al. Epidemio-Clinical and Paraclinical Aspects of Venous Thromboembolic Diseases in a Cardiology Department in Mali. Cardiol. Cardiovasc. Res. 2024, 8(2), 73-77. doi: 10.11648/j.ccr.20240802.14
AMA Style
Mamadou T, Adiaratou TC, Daouda F, Hamma S, Mariam D, et al. Epidemio-Clinical and Paraclinical Aspects of Venous Thromboembolic Diseases in a Cardiology Department in Mali. Cardiol Cardiovasc Res. 2024;8(2):73-77. doi: 10.11648/j.ccr.20240802.14
@article{10.11648/j.ccr.20240802.14,
author = {Toure Mamadou and Thiam Coumba Adiaratou and Fofana Daouda and Sankare Hamma and Dagnogo Mariam and Traore Ousmane and Yalcoue Djamila and Guire Sadik Mahamat and Sidibe Samba and Diall Mahan Ameri and Sow Mady and Cisse Almadane and Keita Asmaou and Daffe Sanoussy and Konate Massama and Coulibaly Souleymane and Menta Ichaka},
title = {Epidemio-Clinical and Paraclinical Aspects of Venous Thromboembolic Diseases in a Cardiology Department in Mali
},
journal = {Cardiology and Cardiovascular Research},
volume = {8},
number = {2},
pages = {73-77},
doi = {10.11648/j.ccr.20240802.14},
url = {https://doi.org/10.11648/j.ccr.20240802.14},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ccr.20240802.14},
abstract = {Introduction: Venous thromboembolic diseases (VTED) include deep vein thrombosis of the lower limbs and pulmonary embolism (PE), which is its severe form due to its high mortality. The objective of our study was to determine the epidemio-clinical and paraclinical aspects of patients hospitalized for venous thromboembolic diseases. Patients and method: Cross-sectional study with prospective recruitment from patient records hospitalized for (VTED) from January to December 2023 in the cardiology department of the Mother-Child University Hospital in Bamako, Luxembourg. Results: We collected 55 out of 580 patient records hospitalized for (VTED), a hospital frequency of 9.48%. PE accounted for 58.20% of cases, 10.90% for deep vein thrombosis (DVT), and 30.90% for their association. The mean age of patients was 55.56 years ± 15.52 years. The majority of patients, 90%, were under 66 years of age. The predominance was female, 56%. In lower extremity DVT, calf pain and Homans' sign were present in 56% and 24% of patients. In pulmonary embolism, dyspnea and chest pain were present in 85.50% and 65.50% of patients. Etiological factors were dominated by neoplasia in 10.90%, contraception 5.45% and orthopedic surgery in 5.45% of cases. Cardiovascular risk factors were a sedentary lifestyle (50.90%), obesity (34.45%), high blood pressure (36.36%) and diabetes (21.81%). Laboratory abnormalities were elevation of troponin (46.87%), BNP (40.62%), D-Dimer (62.50%) and anemia (9.09%). Electrocardiographic abnormalities were tachycardia in 65.4% and S1Q3 in 21.81% of patients. Echocardiography showed dilation of the right cavities (47.27%), systolic pulmonary arterial hypertension (38.18%) and thrombus in the right cavitary (5.45%). On thoracic CT angiography, PE was proximal (36.40%), bilateral (61.80%) and massive (29.10%). On venous Doppler ultrasound, TVP was proximal in 65.21%. Conclusion: VETD was more common in women and younger subjects.
},
year = {2024}
}
TY - JOUR T1 - Epidemio-Clinical and Paraclinical Aspects of Venous Thromboembolic Diseases in a Cardiology Department in Mali AU - Toure Mamadou AU - Thiam Coumba Adiaratou AU - Fofana Daouda AU - Sankare Hamma AU - Dagnogo Mariam AU - Traore Ousmane AU - Yalcoue Djamila AU - Guire Sadik Mahamat AU - Sidibe Samba AU - Diall Mahan Ameri AU - Sow Mady AU - Cisse Almadane AU - Keita Asmaou AU - Daffe Sanoussy AU - Konate Massama AU - Coulibaly Souleymane AU - Menta Ichaka Y1 - 2024/05/30 PY - 2024 N1 - https://doi.org/10.11648/j.ccr.20240802.14 DO - 10.11648/j.ccr.20240802.14 T2 - Cardiology and Cardiovascular Research JF - Cardiology and Cardiovascular Research JO - Cardiology and Cardiovascular Research SP - 73 EP - 77 PB - Science Publishing Group SN - 2578-8914 UR - https://doi.org/10.11648/j.ccr.20240802.14 AB - Introduction: Venous thromboembolic diseases (VTED) include deep vein thrombosis of the lower limbs and pulmonary embolism (PE), which is its severe form due to its high mortality. The objective of our study was to determine the epidemio-clinical and paraclinical aspects of patients hospitalized for venous thromboembolic diseases. Patients and method: Cross-sectional study with prospective recruitment from patient records hospitalized for (VTED) from January to December 2023 in the cardiology department of the Mother-Child University Hospital in Bamako, Luxembourg. Results: We collected 55 out of 580 patient records hospitalized for (VTED), a hospital frequency of 9.48%. PE accounted for 58.20% of cases, 10.90% for deep vein thrombosis (DVT), and 30.90% for their association. The mean age of patients was 55.56 years ± 15.52 years. The majority of patients, 90%, were under 66 years of age. The predominance was female, 56%. In lower extremity DVT, calf pain and Homans' sign were present in 56% and 24% of patients. In pulmonary embolism, dyspnea and chest pain were present in 85.50% and 65.50% of patients. Etiological factors were dominated by neoplasia in 10.90%, contraception 5.45% and orthopedic surgery in 5.45% of cases. Cardiovascular risk factors were a sedentary lifestyle (50.90%), obesity (34.45%), high blood pressure (36.36%) and diabetes (21.81%). Laboratory abnormalities were elevation of troponin (46.87%), BNP (40.62%), D-Dimer (62.50%) and anemia (9.09%). Electrocardiographic abnormalities were tachycardia in 65.4% and S1Q3 in 21.81% of patients. Echocardiography showed dilation of the right cavities (47.27%), systolic pulmonary arterial hypertension (38.18%) and thrombus in the right cavitary (5.45%). On thoracic CT angiography, PE was proximal (36.40%), bilateral (61.80%) and massive (29.10%). On venous Doppler ultrasound, TVP was proximal in 65.21%. Conclusion: VETD was more common in women and younger subjects. VL - 8 IS - 2 ER -
Cardiology Department, CHU-Mother Child, Bamako, Mali; Cardiology Department, CHU-Gabriel Touré, Bamako, Mali; Faculty of Medicine, University of Sciences, Techniques and Technologies of Bamako, Bamako, Mali
Cardiology Department, CHU-Mother Child, Bamako, Mali; Cardiology Department, CHU-Gabriel Touré, Bamako, Mali
Cardiology Department, CHU-Mother Child, Bamako, Mali